
For many women and couples trying to conceive, the journey can feel like an emotional rollercoaster. If you’ve undergone fertility testing or treatment and been told you’re a “low responder,” it’s understandable to feel discouraged. But being a low responder during IVF doesn’t mean your dream of having a baby is out of reach. With the right protocol and expert guidance in reproductive medicine, there is still hope.
In this guide, we’ll walk you through what it means to be a low responder, what causes a poor ovarian response, and the options available that are designed specifically for IVF poor responders.
What Is a Low Responder in IVF?
Medical Definition of a Low Responder
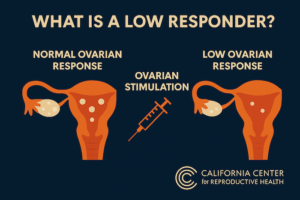
A “low responder” in IVF refers to someone whose ovaries produce fewer eggs than expected in response to ovarian stimulation. This is often diagnosed during or after an IVF cycle, when the number of oocytes retrieved is lower than anticipated.
Clinically, the ESHRE Bologna criteria define poor responders as patients meeting at least two of the following:
- Advanced maternal age (≥40 years).
- Previous poor ovarian response (≤3 oocytes with conventional stimulation).
- Abnormal ovarian reserve tests (e.g., low AMH or low antral follicle count).
Common Indicators and Risk Factors
Several factors can contribute to a poor response during IVF:
- Advanced maternal age: Egg quantity and quality decline with age.
- Low ovarian reserve: Often measured via AMH levels, antral follicle count, or FSH levels.
- Previous ovarian surgery: Can reduce ovarian tissue and blood flow.
- Genetic predispositions or autoimmune conditions.
- Lifestyle factors: Smoking, stress, or being underweight/overweight.
Emotional Toll on Patients
Being labeled a poor responder can feel like a heavy blow, especially after months or years of trying to conceive. The emotional toll includes anxiety, frustration, and fear that treatment may not work. However, it’s important to remember that a poor response doesn’t equal no chance. Many women in this category have gone on to have successful pregnancies with personalized care and the right approach in reproductive medicine.

Why Does a Low Ovarian Response Happen?
Role of Hormones in Follicular Development
During a typical IVF cycle, medications stimulate the ovaries to produce multiple eggs. These medications often include gonadotropins, which contain follicle stimulating hormone (FSH) and luteinizing hormone (LH).
Poor ovarian responders may have:
- Ovaries that don’t respond adequately to ovarian stimulation.
- Hormonal imbalances that impair follicle development.
- A limited number of follicles to begin with.
Low Ovarian Reserve vs. Ovarian Failure
While these terms are sometimes used interchangeably, they describe different scenarios:
- Low ovarian reserve: Fewer eggs available, but still capable of producing a response with the right stimulation strategy.
- Ovarian failure: Complete loss of ovarian function, usually requiring donor eggs.
Understanding the difference is crucial for choosing the right fertility treatment.
IVF Options for Poor Responders
Ovarian Stimulation Protocols Tailored for Poor Responders
| Protocol Type | Medication Dose | Cycle Duration | Typical Candidates | Pros | Cons |
|---|---|---|---|---|---|
| Mild Stimulation | Low dose gonadotropins + oral agents (e.g. letrozole, clomiphene) | Shorter (8–10 days) | Poor responders, advanced maternal age, or those with low ovarian reserve | Lower medication cost, reduced risk of ovarian hyperstimulation | Fewer oocytes retrieved, potentially lower cumulative success |
| Conventional Stimulation | High dose gonadotropins (FSH, LH) | 10–14 days | Patients with normal ovarian reserve or unknown prognosis | Higher oocyte yield, higher chance of embryos per cycle | Higher cost, risk of ovarian hyperstimulation, more side effects |
| Antagonist Protocol | Flexible gonadotropin dose + GnRH antagonist | 8–12 days | Poor responders or those at risk of poor response or early LH surge | Personalized dosing, shorter cycle, better control over LH surge | Requires close monitoring, response still may be suboptimal |
For women diagnosed as low responders, choosing the right stimulation protocol is essential. Some of the most effective approaches include:
- Antagonist protocol is flexible protocol that allows lower hormone doses while preventing premature ovulation – often used for poor responders who need a gentler, more adaptive approach. This strategy has been shown to be particularly effective in patients with poor ovarian reserve.
- Microdose flare protocol uses low doses of GnRH agonists to stimulate a stronger response in ovaries that are otherwise less responsive.
- DuoStim (dual stimulation) stimulates the ovaries twice in one menstrual cycle (follicular and luteal phase), increasing the number of eggs retrieved in a shorter time frame. A recent study found this method significantly increased the egg yield in low responder patients.

Conventional vs. Mild Stimulation: Which Works Best?
Conventional stimulation uses higher doses of gonadotropins, aiming to retrieve as many eggs as possible. However, in poor responders, this doesn’t always lead to better outcomes and can increase the risk of ovarian hyperstimulation.
According to a guideline published by the ASRM, mild ovarian stimulation protocols in poor responders can offer similar pregnancy rates compared to conventional high-dose approaches, but with lower cost and less stress on the body.
The Importance of Personalization in Treatment
No two patients are the same, and for poor responders, personalization is key. Fertility clinics may now use:
- AI-driven stimulation planning to predict the best protocol for each ovarian stimulation cycle.
- Pharmacogenomic testing to assess how patients metabolize fertility drugs.
- Detailed hormonal profiling to improve response to ovarian stimulation.
A 2014 study emphasized the importance of tailoring treatment based on individual hormonal and ovarian reserve profiles to improve outcomes in poor responders. The goal is to create a protocol tailored to your body’s unique hormone levels and reproductive goals.
Success Rates and What to Expect
How Many Eggs Are Enough?
While typical IVF cycles aim for 10-15 eggs, success is still possible with fewer:
- Studies show that even 1-2 high-quality embryos can result in pregnancy.
- Quality matters more than quantity, especially for women with diminished reserves.

Success Rates for Poor Responders Undergoing IVF
Success rates vary based on age, low ovarian response, and the stimulation protocol used:
- Women under 35 with a poor response may still see promising outcomes.
- For those over 40 with poor ovarian reserve, success may require multiple IVF treatments or alternative strategies such as egg donation.
The key takeaway is that poor ovarian response doesn’t mean zero chance – it just means a different approach may be necessary.
Emotional and Financial Considerations
Poor responders often face a higher emotional and financial burden due to:
- The possibility of multiple IVF treatments.
- Lower success per cycle.
- Limited or no insurance coverage.
Support from a fertility counselor and a clear financial plan can help manage the journey. Some clinics offer multi-cycle discount packages or refund programs tailored for poor responders.
Complementary and Alternative Approaches
Supplements and Nutritional Support
Several supplements may help improve egg quality and ovarian response:
- DHEA: May support androgen levels and increase follicle count.
- CoQ10: Enhances mitochondrial function in eggs.
- Antioxidants: Protect egg cells from oxidative stress.
Always consult your fertility doctor before starting supplements.
Lifestyle Changes to Improve Ovarian Response
Simple lifestyle adjustments may enhance fertility outcomes:
- Adopt a Mediterranean-style diet rich in whole grains, healthy fats, and lean proteins.
- Reduce alcohol and caffeine intake.
- Prioritize sleep and stress management.
- Maintain a healthy weight through moderate exercise.
These changes support overall hormonal balance and reproductive health.
When to Consider Other Fertility Treatments
When IVF Isn’t Enough
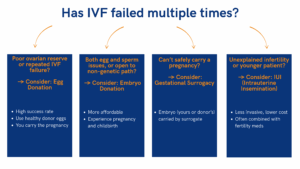
In cases where multiple IVF attempts fail, your doctor may suggest alternative paths:
- Egg donation: For women with extremely poor ovarian reserve, ovarian failure, or repeated IVF failure, egg donation offers one of the highest success rates in assisted reproductive technology. Donor eggs come from healthy, screened women (usually under 30) and are fertilized with your partner’s or donor sperm, then transferred to your uterus. While emotionally complex, this option allows for pregnancy, childbirth, and the early nurturing bond with your child.
- Embryo donation: This involves adopting surplus embryos from another couple’s IVF. It can be more affordable than egg donation and allows patients to experience pregnancy and birth, even if the genetic link isn’t present. Embryo donation is ideal for couples facing both egg and sperm-related challenges or for those open to alternative family-building paths.
- Gestational surrogacy: In cases of repeated implantation failure, uterine abnormalities, or medical conditions preventing safe pregnancy, gestational surrogacy may be recommended. Your embryo (created with your egg or a donor’s) is transferred to a surrogate’s uterus, allowing you to become a parent when carrying the pregnancy isn’t possible.
- Intrauterine insemination (IUI): For select low responder patients with regular ovulation and open fallopian tubes, intrauterine insemination may be considered before IVF. While IUI typically has lower success rates than IVF, it can be combined with gonadotropin stimulation to enhance follicle development and improve the odds of conception in younger patients or those with unexplained infertility.
While these options may be emotionally difficult, they offer excellent success rates and the opportunity to build a family.
Navigating Complex Reproductive Decisions
Choosing the next step can be overwhelming. Many couples benefit from:
- Fertility counseling.
- Second opinions from reproductive endocrinologists.
- Support groups or online communities.
Being informed and supported empowers you to make the best decisions for your journey to parenthood.
Start Your Personalized IVF Plan with Experts Who Understand Low Responders
Facing a low ovarian response or being labeled a poor responder can be overwhelming – but it doesn’t mean your journey to parenthood is over. Advances in reproductive medicine, personalized ovarian stimulation protocols, and evolving approaches like antagonist protocols and gonadotropin stimulation are improving outcomes every year.
If you’re struggling with fertility and wondering which approach is right for you, our clinic specializes in treating low response patients. Let’s find a treatment plan tailored to your unique biology and fertility goals. Schedule a consultation with our fertility specialists today and take the next step toward building your family with confidence!

Eliran Mor, MD
Reproductive Endocrinologist located in Encino, Valencia & West Hollywood, CA
Reproductive Endocrinologist located in Encino, Valencia & West Hollywood, CA Doctor Mor received his medical degree from Tel Aviv University-Sackler School of Medicine in Israel. He completed a four-year residency in Obstetrics and Gynecology at New York Methodist Hospital in Brooklyn, New York. Subsequently, Dr. Mor completed a three-year fellowship in Reproductive Endocrinology and Infertility […]


